When someone in your family is diagnosed with multiple myeloma, one of the first questions that comes up is simple and deeply personal:
Is multiple myeloma hereditary?
It’s a fair question. And it deserves a clear, calm answer.
Is Multiple Myeloma Hereditary?
Most cases of multiple myeloma are not directly inherited from a parent.
However, having a close family member with multiple myeloma can slightly increase your risk.
That does not mean you will develop it. It means awareness matters.
Let’s break that down in plain language.
What Multiple Myeloma Is
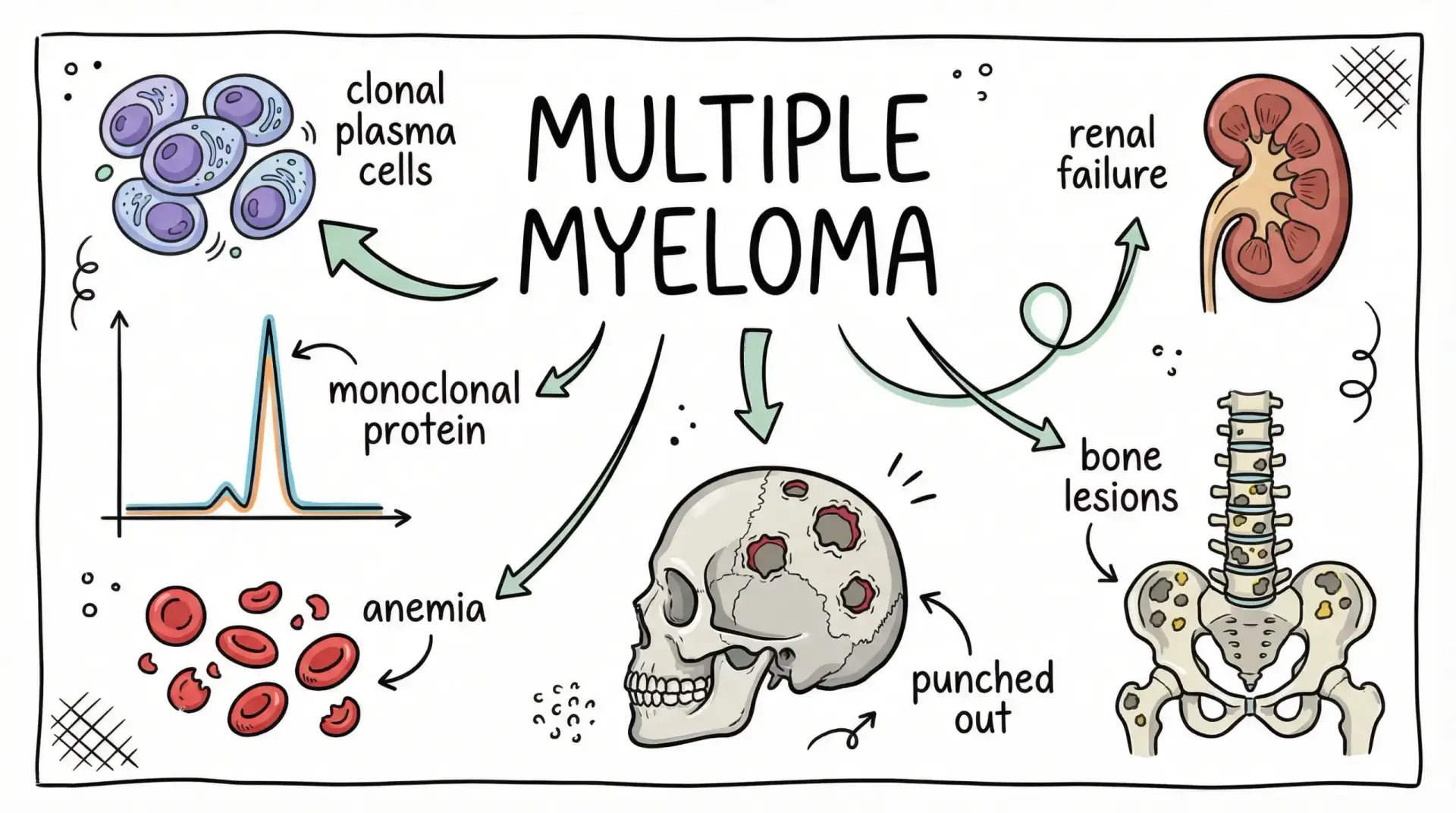
Multiple myeloma is a cancer of plasma cells, a type of white blood cell found in your bone marrow. Plasma cells help your body fight infection.
Yes — multiple myeloma is a blood cancer.
People often ask about heredity because:
- Cancer can cluster in families.
- We share genes with our parents and siblings.
- We share environments and lifestyle patterns.
- Hearing “genetic changes” sounds like “inherited.”
But those terms don’t always mean the same thing.
Is Multiple Myeloma Hereditary or Genetic?
Here’s the key distinction:
- Hereditary means passed directly from parent to child through inherited genes.
- Genetic means involving changes in DNA — but those changes often happen over time and are not inherited.
According to the American Cancer Society and MedlinePlus Genetics, multiple myeloma usually develops due to acquired DNA changes in plasma cells during a person’s lifetime — not because a parent passed down a specific gene mutation.
However, having a first-degree relative (parent, sibling, child) with multiple myeloma does increase your risk compared to someone without that history.
- The overall risk of multiple myeloma in the general population is still relatively low.
- Even with family history, most people never develop it.
Family history raises risk — it does not guarantee disease.
How Common Is Multiple Myeloma in Texas?
According to official data from the Texas Cancer Registry and the CDC’s U.S. Cancer Statistics program, multiple myeloma represents a small percentage of all cancer diagnoses.
Incidence rates are typically reported as cases per 100,000 people and increase significantly with age. Rates are higher among:
- Adults over 65
- Males
- Black/African American individuals
Local county-level data (including Harris County) can vary slightly year to year, and smaller counts may be statistically suppressed in some datasets.
Multiple myeloma is not common in younger adults. Risk increases with age.
Symptoms of Multiple Myeloma: Early vs. Later Signs

One reason this topic matters in an ER setting is that multiple myeloma often presents with symptoms that are easy to dismiss at first.
Early Symptoms
- Fatigue that doesn’t improve with rest
- Mild anemia symptoms (feeling weak, short of breath with exertion)
- Recurring infections
- Vague bone aches
These can look like dehydration, aging, stress, or back strain.
Later Symptoms
- Persistent bone pain (especially back, ribs, hips)
- Unexplained fractures
- Frequent infections
- Unusual bruising or bleeding
- Unintentional weight loss
- Nausea, constipation, excessive thirst
- Mental fog or confusion
These happen because the disease can affect:
- Bone strength
- Red blood cell production
- Kidney function
- Calcium levels
Who Is More at Risk?
Multiple myeloma risk increases with:
- Age (most diagnoses occur after 65)
- Male sex
- Black/African American race
- Family history of multiple myeloma
- Personal history of MGUS (monoclonal gammopathy of undetermined significance)
- Obesity
But remember: risk factors are not causes. Many people with risk factors never develop myeloma.
Go to the ER Now If You Notice These Symptoms
While family history alone is not an emergency, certain symptoms are.
Seek immediate emergency care if you experience:
- Chest pain or trouble breathing
- Fainting or extreme weakness
- New confusion or severe drowsiness
- High fever with shaking chills
- Severe back pain with numbness, weakness, or loss of bowel/bladder control
- Sudden fracture after minor injury
- Very low urine output, severe swelling, or uncontrolled vomiting
These could signal serious complications such as:
- Severe anemia
- Kidney failure
- Spinal cord compression
- High calcium levels
- Severe infection
If you or a loved one have severe weakness, confusion, chest pain, trouble breathing, or sudden worsening symptoms, don’t wait. Post Oak ER is open 24/7 for immediate emergency evaluation and care.
What Doctors May Do Next
If symptoms bring you to the ER, the focus is stabilization and evaluation.
Doctors may order:
- Blood tests (complete blood count, kidney function, calcium levels)
- Imaging studies (if severe bone pain or fracture is suspected)
- Infection screening
- Urgent specialty referral if needed
The ER does not replace oncology care, but it plays a critical role when complications arise.
What You Can Do Today
If you’re concerned because of family history:
- Keep a record of which relative had multiple myeloma and at what age.
- Share that information with your primary care provider.
- Ask whether routine blood work is appropriate for you.
If you’re concerned because of symptoms:
- Track how long symptoms have been present.
- Note what is worsening.
- Don’t self-diagnose based on internet searches.
- Let severity guide urgency.
And if you feel unsafe or severely ill — don’t wait.
Frequently Asked Questions
Does multiple myeloma run in families?
It can cluster in families, but it is not typically inherited in a simple pattern. Having a close relative slightly increases risk.
Is multiple myeloma genetic or inherited?
It involves genetic changes in plasma cells, but those changes usually occur during life rather than being inherited at birth.
If my parent has multiple myeloma, what is my risk?
Your risk is higher than someone without family history, but still relatively low overall. Most people with a family history never develop it.
Should family members get genetic testing or screening?
Routine genetic testing is not standard for most families. If you’re concerned, discuss risk assessment with your primary care provider.
What are the early warning signs of multiple myeloma?
Fatigue, recurrent infections, and persistent bone pain are common early symptoms — but they are nonspecific. Persistent or worsening symptoms should be evaluated.
What symptoms mean you should go to the ER immediately?
Severe weakness, confusion, chest pain, high fever, severe back pain with neurological symptoms, or signs of kidney failure should be treated as emergencies.