If you or someone you love has been told “you may need dialysis,” it can feel like the ground shifts under your feet. Dialysis is a treatment that does part of the work your kidneys can’t do anymore—filtering waste and extra fluid—when kidney failure is advanced.
CDC notes that more than 1 in 7 U.S. adults may have chronic kidney disease (CKD), and as many as 9 in 10 don’t know they have it.
For some people, CKD progresses to kidney failure—where dialysis or transplant becomes necessary to survive.
Educational only. Not a diagnosis or personal medical advice.
What is dialysis, in plain English?
Dialysis is a medical treatment that helps your body by:
- removing waste products your kidneys normally filter out
- removing extra fluid that can build up in the body
- helping maintain a safer balance of minerals and electrolytes
Does dialysis cure kidney failure?
No—dialysis is not a cure, but it can help you feel better and live longer.
NIDDK also explains that none of the kidney failure treatment options (dialysis, transplant, or conservative management) make the kidneys “get better,” but they can help you feel better.
Who needs dialysis (and when does it happen)?
Dialysis is used for kidney failure (often called end-stage kidney disease).
Many people live for years with earlier-stage CKD (like Stage 3 or Stage 4) without dialysis. Dialysis becomes part of the conversation when kidney function is severely reduced and symptoms, labs, or fluid/electrolyte issues indicate the body needs help.
The main types of dialysis

National Kidney Foundation explains there are three main dialysis categories:
- In-center hemodialysis
- Home hemodialysis
- Peritoneal dialysis
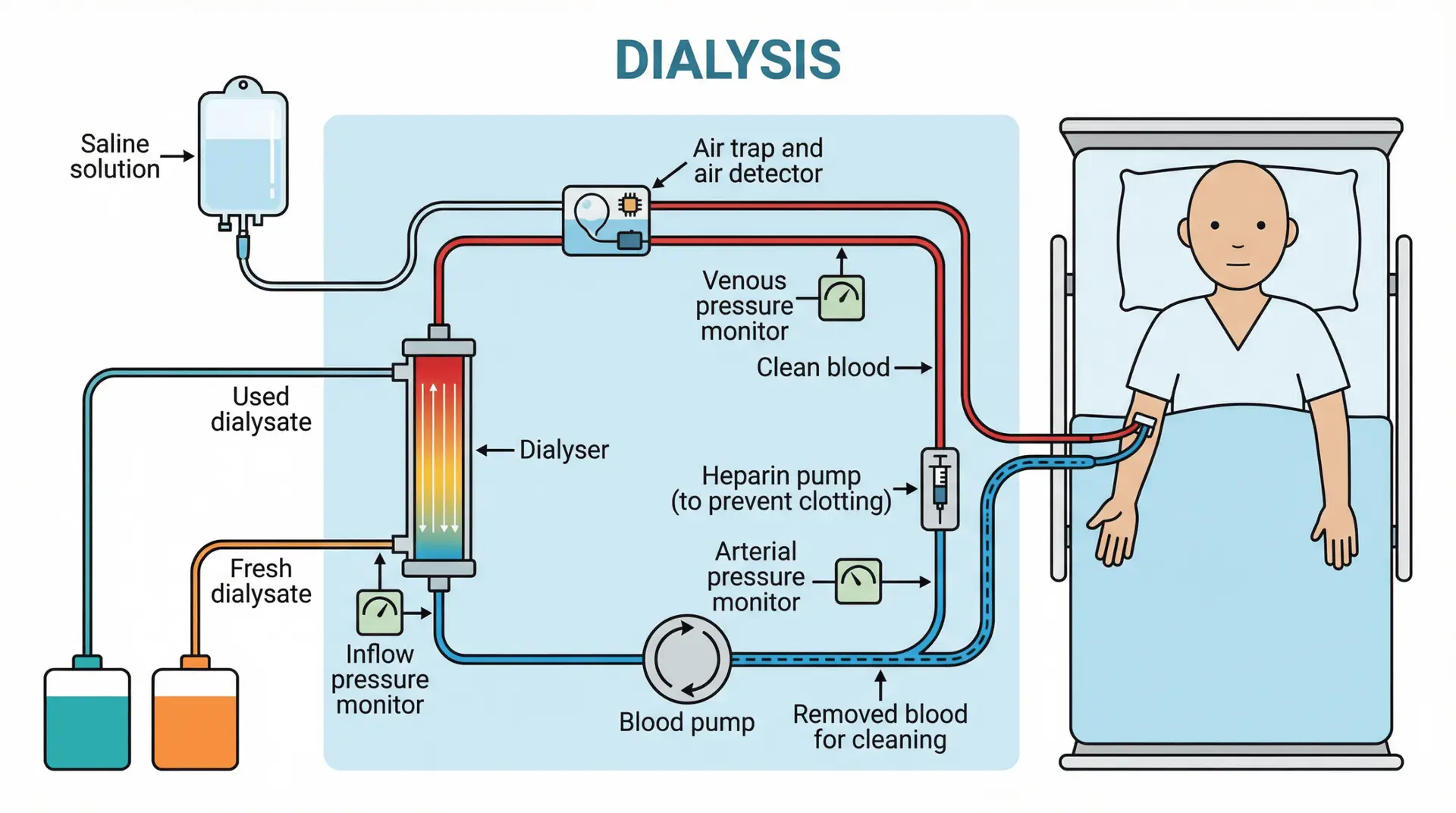
Hemodialysis (blood is filtered outside the body)
NIDDK explains that during hemodialysis, blood goes through a filter (dialyzer) outside the body.
NKF describes hemodialysis as a life-saving treatment that removes waste/extra fluid and helps regulate blood pressure.
Access matters: Before regular hemodialysis, most patients need a vascular access (often a fistula or graft), and NIDDK calls that access your “lifeline.”
How often is hemodialysis needed—and how long does it take?
For most people, hemodialysis happens three times per week, with each session lasting about four hours. This is the typical schedule recommended by organizations like the National Kidney Foundation and NIDDK to help keep waste and extra fluid in check when the kidneys are no longer up to the task. The exact frequency and length may be tailored based on your individual health, but this “three times a week, four hours each” setup is what many patients can expect.
What safety steps are taken at dialysis centers?
Health and safety are front and center at dialysis clinics. The CDC and the National Kidney Foundation both outline thorough protocols to help keep patients, visitors, and staff as protected as possible—especially since many dialysis patients have higher risks for infections.
Here’s what you can generally expect:
- Enhanced cleaning: Equipment and surfaces are routinely disinfected before and after each session.
- Screening: Staff and patients are screened for symptoms, and anyone who might be sick is often asked to reschedule or follow special procedures.
- Hand hygiene: Washing and sanitizing hands before and after patient contact is strictly enforced.
- Face masks and PPE: Masks (and in many cases, additional protective gear) are worn by staff and frequently by patients, following the latest public health guidance.
- Distancing measures: Waiting rooms and treatment areas are often reconfigured to help everyone keep a safe distance.
These steps are designed with your wellbeing in mind—dialysis centers work hard so that treatment environments remain as safe and welcoming as possible for every visit.”
Peritoneal dialysis (PD) (filtering happens inside the body)
NIDDK explains PD uses the lining of the abdomen (the peritoneum) to filter blood inside the body, using dialysis solution that flows in and out through a catheter. During peritoneal dialysis, this special fluid (called dialysate) is put into the abdominal cavity through a catheter. The peritoneum acts as a natural filter—removing waste and extra fluid from your blood as the solution sits, or “dwells,” inside your belly for a set amount of time. After the dwell time, the fluid—now containing the filtered waste products—flows back out through the catheter and is discarded.
Types of PD (NIDDK):
- CAPD (manual exchanges during the day)
- Automated peritoneal dialysis (cycler machine while you sleep)
A practical scheduling detail: NIDDK notes CAPD exchanges typically take 30–40 minutes, dwell time is often 4–6 hours or more, and people usually do exchanges at least four times a day.
NIDDK also notes automated PD can do exchanges three to five times during the night with a cycler.
Automated Peritoneal Dialysis: How It Works
Automated peritoneal dialysis—sometimes called continuous cycling peritoneal dialysis (CCPD)—uses a machine that cycles through multiple exchanges while you sleep. The machine fills your abdomen with dialysate, lets it dwell for a set period, and then drains it into a sterile bag. You’ll typically remain connected to the machine for about 10–12 hours overnight. In the morning, you disconnect and can go about your day, with the final fill staying in your abdomen as a daytime dwell until you reconnect that night.
This overnight approach means you’re generally free from the machine during the day, making automated PD a flexible option for many people.
Where PD can be done: NIDDK states PD can be done in clean private places—including home, work, or while traveling (with planning for supplies).
Peritoneal dialysis (PD) is a flexible treatment option for those with kidney failure, offering a level of independence not always possible with other forms of dialysis. Unlike hemodialysis, which relies on an artificial kidney machine to filter your blood, PD uses your own abdominal lining—the peritoneum—as a natural filter.
During PD, a cleansing fluid called dialysate flows into your abdomen through a soft tube (catheter). While the fluid is in your belly, the peritoneum removes waste and extra fluid from your blood. After a prescribed “dwell” time, the used dialysate, now containing these filtered wastes, is drained and discarded.
There are two types of PD to consider:
Continuous Ambulatory Peritoneal Dialysis (CAPD)
With CAPD, you fill your abdomen with dialysate and let it dwell for several hours. Exchanges—removing the used fluid and adding fresh—are done by hand, typically three to five times during the day. A longer exchange is performed overnight. Since no machine is needed, you can perform exchanges in any clean, private location, and most daily activities can continue while the dialysate dwells.
Automated Peritoneal Dialysis (APD)
APD, also called continuous cycling peritoneal dialysis (CCPD), uses a machine to automatically perform several exchanges while you sleep. The machine fills and drains your abdomen with dialysate throughout the night; in the morning, you disconnect and start your day with a final daytime dwell.
Both methods allow for treatment to fit into your lifestyle—whether you’re at home, at work, or even traveling, as long as you have a clean space and have made arrangements for your supplies.
While peritoneal dialysis (PD) offers flexibility and the convenience of being done at home or other clean environments, it isn’t suitable for everyone. According to the National Kidney Foundation and NIDDK, some people may not be good candidates for PD, including:
- Those with extensive scarring in the abdomen (often from multiple surgeries)
- People with large hernias or certain abdominal conditions
- Individuals with significant obesity, which can make the treatment less effective or more difficult
- Anyone unable to care for the catheter site safely, or lacking the dexterity or support needed for home-based care
Your care team will consider your overall health, lifestyle, and any surgical history before recommending PD or other options.
How common is PD? Cleveland Clinic notes peritoneal dialysis is the least common dialysis type and estimates about 10% of people who need dialysis receive PD.
How do people choose the “right” dialysis?
This is a personal decision—and it’s normal to revisit it.
National Kidney Foundation emphasizes that each dialysis type has pros/cons and you can often change modalities over time, so you don’t have to feel “locked in.”
NIDDK also encourages learning about options early and working with your care team to build a plan before dialysis is urgently needed.
In real life, the choice often comes down to:
- your overall health and other conditions
- your home setup/support
- your work/life schedule
- whether home therapy is realistic and safe
- what your nephrology team recommends
Both hemodialysis and peritoneal dialysis have features that may make one a better fit than the other for you:
- Peritoneal dialysis offers continuous filtration and can be less disruptive to your daily activities, making it appealing for those seeking more flexibility or independence. However, it requires patient training and a willingness to manage your own treatments. It may not be the best option if you have significant abdominal scarring or are living with obesity.
- Hemodialysis is sometimes preferred for people with less kidney function or for those who would rather have healthcare professionals handle most of the treatment process. For many, the routine and support at a dialysis center feel reassuring.
If your lifestyle or medical needs change, it’s often possible to switch from one type of dialysis to another. The “right” fit can shift over time—and that’s normal. Working together with your care team helps ensure you have the information and support to make the best choice for your life and health.
Common dialysis questions
“Does dialysis hurt?”
Most people don’t describe dialysis itself as “painful,” but it can be uncomfortable—especially early on—because it’s a major change for your body and routine. NIDDK notes adjusting to dialysis and kidney failure can be hard, and diet/fluid changes may be needed.
“What side effects can happen?” (hemodialysis)
NIDDK lists possible issues like:
- muscle cramps
- a sudden drop in blood pressure (hypotension), which can cause weakness, dizziness, or nausea
“Why do dialysis patients have fluid limits?”
NIDDK explains fluid can build up in the body between hemodialysis treatments, and many patients need to limit sodium and fluids.
“Can I travel while on dialysis?”
NIDDK notes PD can be done while traveling with planning (including shipping supplies to where you’re going).
For hemodialysis, travel is possible but typically requires scheduling treatments at a dialysis center at your destination (your dialysis team helps coordinate).
Warning symptoms that shouldn’t wait

Dialysis patients can get sick quickly when something is “off.” Consider urgent evaluation if you have any of the following:
- Chest pain, severe shortness of breath, fainting, or confusion (these are emergency-level symptoms regardless of kidney history)
- Signs of infection at your dialysis access (warmth, redness, drainage, worsening pain). NIDDK specifically advises checking access sites for warmth/redness and notifying your center if you can’t feel the vibration over the access.
- Persistent vomiting or inability to keep fluids down (risk of dehydration and dangerous electrolyte shifts)
- Sudden, significant swelling or worsening shortness of breath (can suggest fluid overload)
- You missed dialysis and feel rapidly worse (severe weakness, shortness of breath, chest discomfort, severe nausea)
If you’re ever uncertain, it is safer to be evaluated than to wait.
If you’re in Houston—especially near Uptown, the Galleria area, the Energy Corridor, Westchase, Midtown, or the Heights—and you’re dealing with warning symptoms that shouldn’t wait, getting checked promptly is reasonable.
Post Oak ER states it is open 24/7 and located right off San Felipe St. near The Galleria and Uptown Park, making it accessible from multiple Houston areas.
They also state they have on-site lab testing and imaging (CT, X-ray, ultrasound) available.